Crohn’s disease | Ulcerative colitis | |
Possible etiology | Postinfectious | Autoimmune |
Location | Any portion of the GI tract, usually the terminal ileum and colon | Continuous colonic lesion, always with rectal involvement |
Gross morphology | Transmural inflammation. Cobblestone mucosa, creeping fat, bowel wall thickening (string sign), linear ulcer, fissures, fistulas | Mucosal and submucosal inflammation only. Friable mucosal pseudopolypos with freely hanging mesentery. “lead pipe” appearance on imaging |
Microscopic morphology | Noncaseating granulomas and lymphoid aggregates | Crypt abscesses and ulcer, bleeding, no granulomas |
Complications | Strictures, fistulas, perianal disease, malabsorption, nutritional depletion | Severe stenosis, toxic megacolon, colorectal carcinoma |
Intestinal manifestation | Diarrhea that may or may not be bloody | Bloody diarrhea |
Extraintestinal manifestation | Migratory polyarthritis, erythema nodosum, ankylosing spondylitis, uveitis, immunologic disorder | Pyoderma grangrenosum, primary sclerosing cholangitis |
Treatment | Corticosteroids, infliximab | ASA products (sulfasalazine), infliximab, 6-mertantopurine |

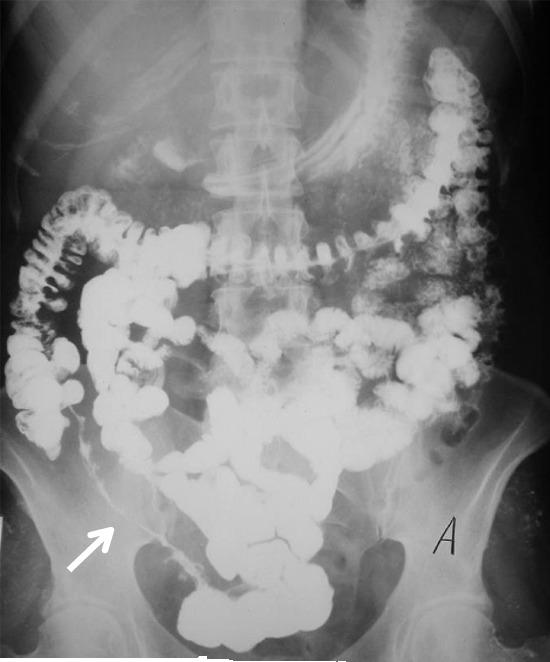
S
tring-sign on barium swallow x-ray
No comments:
Post a Comment